
It took us a little time to figure out how to fit the Coronavirus pandemic into a fully formed political debate. We’ve hit our stride pretty quickly though. It turns out it actually fits neatly into the same sort of debate we’ve always had in American politics.
Coastal elites with their charts and mathematical models and high science degrees are telling everyone else that there’s a giant problem. And while most of them have the sorts of jobs where they make a living in just about any economy, they’ve gone ahead and forced us to do something that’s killed all the higher paying working-class jobs. And they’re hiding behind a “phony” motivation of protecting the most vulnerable Americans in order to do it.
Meanwhile, Joe the plumber, just doesn’t get it. The universe is trying to tell him the world is going to end. And he doesn’t care. All he cares about is himself and people that look like him. All the experts agree but he doesn’t care because he doesn’t understand science. It may be hard on him. But it’s not as hard on him as it is on the truly poor and the elderly. Who are ALL going to die. Why won’t he just listen and do what we tell him to?
Healthcare, globalization, immigration, climate change…now Covid-19.
It’s on.
There’s one critical difference here though. This is not a hypothetical slow burn discussion that requires pundits and politicians to pour gas on it from time to time to keep it going. It’s an acute crisis that will force an outcome, one way or another, in weeks or months…not years or decades.
Over 4,000 Americans have died in the last 24 hours. Most of the deaths are in metropolitan areas like New York. Meanwhile, we’ve got at least 25% unemployment in Michigan. And they’re not alone.
Neither of these issues are sustainable for very long. So, we’ve got some extremely difficult choices that are going to require thinking that can’t be contained by the standard 21st Century American political debate.
It starts by acknowledging that both the problems of a sustained great depression level economic crash and an overwhelming viral pandemic killing thousands of Americans a day are things we can’t live with. We don’t need hyperbolic claims that recessions kill people. And we don’t need people who are urging us to open the economy being called murderers. It’s sufficient to simply say that we can’t trade one outcome for the other. Not for long.
Debates over what’s worse aren’t necessary. Clearly the pandemic is worse because it’s killing thousands of people a day. But it’s worse the way dying of dehydration is worse than starving to death. You can tell people not to eat or they’ll die of thirst for only so long before they go looking for food on their own. The protests are already starting.
Objectively we should all agree that there will be a time when we can start to have an intelligent discussion about when the economic impact begins to outweigh the value of future improvements in public safety. For those folks in the “break a few eggs to make an omelet” camp that think we’re there now, I’ve got a chart originally published by The New Atlantis that can add perspective:
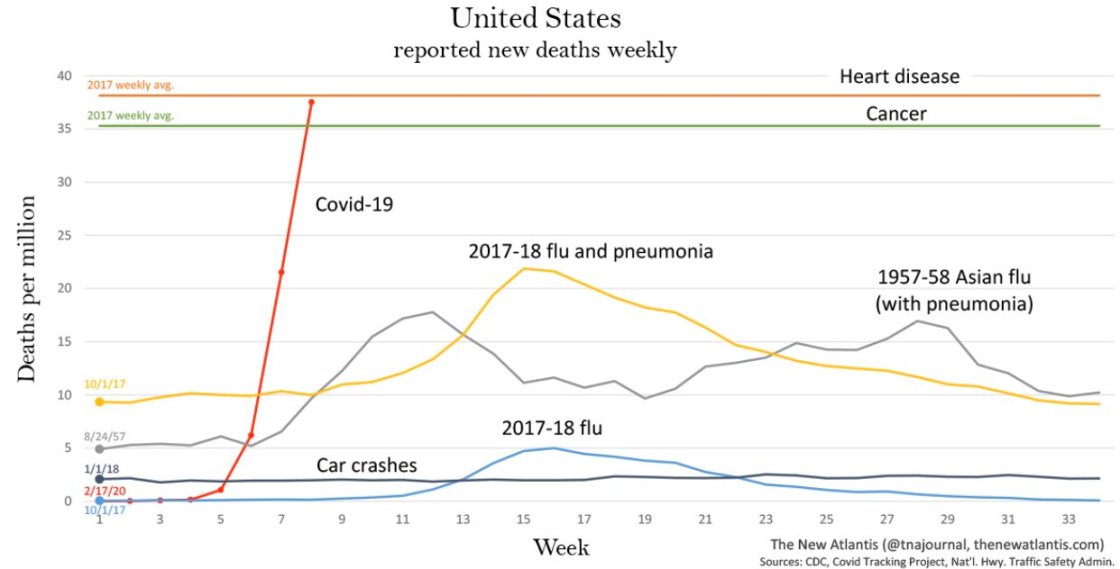
Dr. Phil was right when he went on Fox News and said we don’t close down the economy for car crashes or the flu, both of which kill tens of thousands of Americans a year. As you can see from the chart, Covid-19 is not the flu or car crashes. Or anything we’ve seen since the advent of modern medicine. That curve will flatten out on it’s own at some point…probably… But we’d kill a whole lot of people to find out when. We’ll definately break some eggs. It’s not clear whether or not we’d even have an omelet on the other side though. Which brings up the most critical aspect of our current predicament.
While the Covid-19 weekly death curve looks like that, does it really matter if someone declares the economy open?
Let’s take my hometown of Atlantic City as a case study for this question. It’s a single industry town of casino tourism. Right now all casinos are closed. If Governor Phil Murphy declared the economy “open” at noon today, are people going to the Casino this weekend? Are Americans going to gather in the thousands in small rooms and close seating with senior citizens to gamble?
How about you? Are you going to a crowded restaurant? To the movies? Are you getting on a plane to fly cross country for a work conference you don’t feel like going to?
How about employers? Are they making their staff show up?
Right now over four thousand Cops in New York City have Covid-19. 27 have died. That’s more police officers than died on 9/11. And about 10% of all line of duty related deaths for NYC cops since 1950. In three weeks. You read that right.
Whose excited to bring their teams back together…?
The painful reality is that in many areas, the government hasn’t shut down the economy. The virus has. And for the others, the belief is that it would just be a matter of time before it does so we may as well save lives while we wait it out.
That’s the right strategy. It’s just not complete.
“Stay the fuck home” memes are a fun way to value signal that you’re on team coastal elite. But they don’t do much to help people who don’t know what they’re going to do if we shut down forever. The good news for them is that no one thinks we can shut down forever. The bad news is that no one has provided an alternative reality to look forward to. Which means people are arguing what they know; “open” or “shut”. The future looks like neither, at least not for a little while. So a political debate is not only unhelpful, it’s fundamentally illogical.
This is not a binary political debate. It’s a war. But unlike previous American wars that were fought in far off places bolstered by an American economy that was actually energized to support it, this one is being fought on our soil.
We’re not America in WWII. We’re France…complete with Maginot Line to the south.
We have the brutal task of defeating an external belligerent (the virus) and an internal one (economic collapse) at the same time. It might be an exaggeration to say this is America’s first total war on our soil. But not by much. And we need to fight it that way.
There are three fronts:
1-Fight the disease. Medical capacity, disease containment, therapeutic treatment, and…vaccine.
2-Provide financial sustainment. Over the top, New Deal scope programs that cover people, small businesses and corporations. Don’t make it an either or. Do it all. Do it for as long as we can.
3-Systematically open up society where we can and when we can. Maybe start with schools. Ask questions like what behavioral, technological and organizational innovations would be required to get kids back into school by September?
That’s it. That’s the fight. Anything else is a show.
Be wary of the political/media industrial complex pitching other topics. And be wary of politicians disguised as civic leaders using this war as a platform. If they aren’t talking about any of the three fronts in the war and what they are doing to deliver against them, it’s not worth the time.


